![]()

Almost all patients with ankle sprains will initially have a trial of a boot, bracing, crutches and physical therapy. Most patients will be encouraged to pursue this treatment for at least three months before considering surgery. If you have other injuries such as damage to ankle cartilage, a peroneal tendon tear, and/or certain fractures, you may be encouraged to have surgery sooner. If you have ankle instability for months or years and have already tried bracing and therapy, surgery is something to consider now.
Patients who are candidates for surgery have ankle instability and pain interfering with their life. They have failed bracing and therapy. They are also willing and able to stay off their ankle for at least two weeks after surgery.
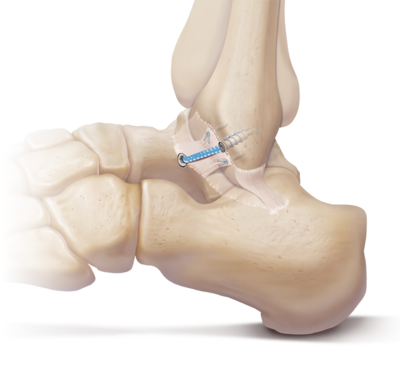
The Brostrom procedure is a method of “tightening” the ankle. The ligaments that keep the ankle stable are torn or have healed too loosely and require repair/tightening. This is accomplished through an incision over the outside of your ankle so that the loose ligaments can be cut. They are then repaired to the correct tension and secured with sutures, or sometimes metal or plastic anchors. An internal device may also be implanted to act as a brace that functions as a “check rein” to speed recovery. This does not require later removal and is not something you should feel. Surgery commonly takes 30-45 minutes and is done on an outpatient basis. If you have other procedures at the same time (ankle arthroscopy, tendon repair, transfer, etc.), the surgery will take longer, and you may be off your ankle for longer. A nerve block may be offered to you before surgery by anesthesiology to make most of your ankle numb and to reduce your need for pain medications.
Once you are deemed a candidate for surgery, preadmission testing is done to confirm you are healthy for surgery. This will include labs and often an electrocardiogram and chest x-ray. We may occasionally need evaluations from your primary care physician or other specialists such as cardiology prior to surgery. Stop smoking at least four weeks prior to surgery to reduce your risk of lung issues after your procedure, and to lower your risk of not healing or having other complications such as nerve injuries.
You will be placed in a splint to hold your ankle in the proper position and to allow the ligaments to heal appropriately. You will not be allowed to place any weight on your ankle, remove the splint or get it wet for the first two weeks. The splint will be removed after two weeks at your first appointment and will be replaced with a walking boot. After transitioning to the boot, you may progressively bear weight. The boot will be converted to a lace-up brace that can be worn with a shoe at four weeks after surgery. You will also start a physical therapy protocol at that time. This is how the tendons that support your ankle “wake up” so that you can be weaned from your brace. Expect to wear the brace until 12 weeks after surgery, at which point you may return to full athletic activity.
Unless other procedures are done at the same time or an internal brace device is implanted, the typical recovery timeframe is as follows:
Weeks 0-2: Keep off the ankle with crutches, knee scooter, etc. Non-removable splint in place, elevate, do not get wet.
Weeks 0-2: Keep off the ankle with crutches, knee scooter, etc. Non-removable splint in place, elevate, do not get wet.
Weeks 2-4: Walking boot in place, weight bear as tolerated (progressively). Start some ankle range of motion. Ok to get wet.
Weeks 4-12: Physical therapy protocol (often 2-3 times per week). Lace-up ankle brace.• Weeks 12+: Return to all activities, athletic play, no brace required (advised to wear initially if high level athlete).
For additional information about treatment, we have included this complete patient eduction sheet as a pdf to view, download and print:
![]()
Muskegon Office
1400 Mercy Drive, Suite 100
Muskegon, Michigan 49444
231-733-1326
Grand Haven Office
1445 Sheldon Road, Suite 200
Grand Haven, Michigan 49417
616-296-9100
Quick Links




