![]()


Our elbow specialists are highly skilled in treating elbow disorders, and include a broad range of expertise developed through personal experience and advanced fellowship training focused on elbow reconstruction, trauma, and sports related injuries.
The biceps muscle originates from two sites on the shoulder blade and attaches just past the elbow on the radial tuberosity of the radius. It functions to flex the elbow and to supinate the forearm or to rotate the palm up. The distal attachment of the biceps can tear when there is a significant or unexpected load across the elbow. Loss of this tendon results in significant strength loss with elbow flexion and supination. When the distal biceps tendon ruptures, surgical repair is recommended in most cases.
For additional information about this condition, we have included this complete patient eduction sheet as a pdf to view, download and print:
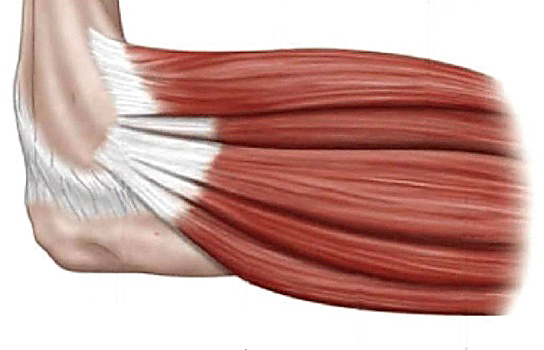
The triceps muscle originates from the upper humerus and shoulder blade and attaches to the olecranon tip at the elbow. It functions to extend or straighten the elbow. Injury to this tendon can result in rupture. This manifests as significant weakness in straightening the elbow. This is the only tendon that extends the elbow and should be surgically repaired if torn.
Arthritis is the loss of the smooth covering over the ends of bones. When this coating is gone, bone rubs on bone and causes inflammation, pain, and decreased range of motion. Arthritis can be caused by ligament injury, previous trauma, or bad luck. Early treatments include therapy exercises, NSAIDs, cortisone injections, and rest. Arthroscopic or open debridement procedures can also help with symptoms if non-operative treatments fail. Total elbow replacement can significantly help with the symptoms, but there is a lifelong lifting restriction of 10 lbs., and there are high rates of revision surgery in younger patients.
The elbow has a tendency to become stiff and lose motion after injury. Loss of some elbow extension is almost guaranteed after significant fractures or dislocations, but even minor injuries can sometimes result in loss of motion. In some instances, the contractures are severe and limit function. In these cases, aggressive physical therapy and stretching are prescribed, in addition to splints that actually “crank” on the elbow to force it straight or into flexion. If non-operative measures do not restore a functional range of motion, sometimes surgery is needed to remove the scarred capsule and other obstructions to elbow movement.
The elbow is stabilized by strong ligaments on the inside (medial aspect) and the outside (lateral aspect). When these ligaments are damaged, it can result in partial dislocations or subluxations of the elbow during certain movements, which causes pain. Repetitive stress (pitching) or trauma (elbow dislocation) can result in disruption of these ligaments. Patients are usually treated with rest and physical therapy at first. If the ligaments do not heal on their own, surgical repair or reconstruction may be necessary.
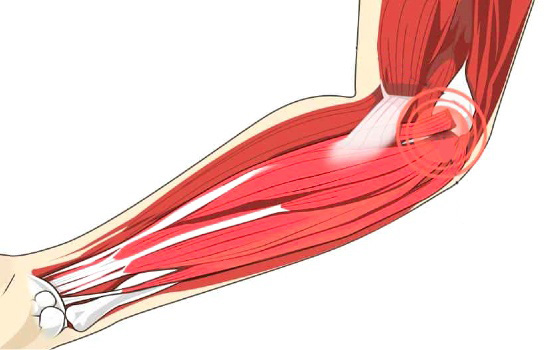
Also termed “tennis elbow,” people with lateral epicondylitis experience pain along the outside of the elbow over the lateral epicondyle. This pain is usually worse with gripping activities or movements involving wrist extension. The forearm muscles that extend the wrist and fingers originate over the lateral epicondyle, and when this tendon attachment becomes inflamed, it results in significant pain. In some cases, it can become painful with even basic activities of daily living. It is initially treated with a combination of rest, ice, NSAIDs, eccentric therapy exercises, and cortisone injections. Surgical debridement and tendon repair may be necessary when non-surgical treatment therapies have not been effective.
For additional information about this condition, we have included this complete patient eduction sheet as a pdf to view, download and print:
Also termed “golfer’s elbow,” people with medial epicondylitis experience pain along the inside of the elbow over the medial epicondyle. This pain is usually worse with gripping activities or movements involving wrist flexion. The forearm muscles that flex the wrist and fingers originate over the medical epicondyle, and when this tendon attachment becomes inflamed, it results in significant pain. In some cases, it can become painful with even basic activities of daily living. It is initially treated with a combination of rest, ice, NSAIDs, eccentric therapy exercises, and cortisone injections. Surgical debridement and tendon repair may be necessary when non-surgical treatment therapies have not been effective.
For additional information about this condition, we have included this complete patient eduction sheet as a pdf to view, download and print:
The bone at the tip of the elbow is called the olecranon, and the tip lies directly under the skin. Between the skin and the bone there is a small fluid filled sac, called the olecranon bursa, which acts as a lubricant between the skin and bone. With repetitive pressure or trauma, this fluid filled sac can become inflamed and fill with more “fluid” than normal. This results in pain and a swelling around the back of the elbow that almost looks and feels like a water balloon. Treatment consists of rest, ice, NSAIDs, and soft braces. Drainage is rarely necessary.
Repetitive impact through the elbow in skeletally immature individuals can result in focal areas of cartilage damage, termed osteochondritis dissecans, or OCD. This generally results in pain, swelling, and decreased range of motion. Cartilage is the smooth, soft, covering over the ends of bones where they articulate. When this covering is damaged, it causes pain. This condition is diagnosed with x-rays and usually an MRI. It is initially treated with rest and NSAIDs. In some cases, surgical debridement or stabilization is required.

Injuries can happen anytime so we have immediate appointments available at our Muskegon and Grand Haven offices. Our orthopaedic urgent care is open to accommodate same day visits for the evaluation of elbow injuries.
![]()
Muskegon Office
1400 Mercy Drive, Suite 100
Muskegon, Michigan 49444
231-733-1326
Grand Haven Office
1445 Sheldon Road, Suite 200
Grand Haven, Michigan 49417
616-296-9100
Quick Links